Vitamin B12, or cobalamin, is a water-soluble vitamin that plays a key role in various physiological processes of the body.
Its uniqueness lies in its complex structure and its indispensability in metabolic pathways. Vitamin B12 deficiency is a global health problem, especially in developed countries, where prevalence can be as high as 20% among the elderly.

Neurologic manifestations of deficiency are often nonspecific and may mimic other diseases, making timely diagnosis difficult. The purpose of this article is to provide a detailed review of the biological role of vitamin B12, causes of its deficiency, neurologic manifestations and modern approaches to diagnosis and treatment.
Biological role of vitamin B12
Vitamin B12 is involved in two major enzymatic reactions in the human body:
-
- Methylation of homocysteine to methionine: The coenzyme form of methylcobalamin is essential for the methionine synthase enzyme, which converts homocysteine to methionine. This process is important for the synthesis of S-adenosylmethionine, the universal methyl donor in the methylation of DNA, RNA and proteins.
- Isomerization of methylmalonyl-CoA to succinyl-CoA: Adenosylcobalamin serves as a cofactor for methylmalonyl-CoA mutase, which converts methylmalonyl-CoA to succinyl-CoA, an important component of the Krebs cycle.
Interesting fact
Vitamin B12 deficiency leads to the accumulation of methylmalonic acid and homocysteine, which can cause neurotoxicity and damage to the myelin sheath of nerve fibers.
Table 1: Vitamin B12 content of some foods
| Product | Vitamin B12 (mcg/100 g) |
|---|---|
| Beef liver | 83 |
| Molluscs | 98 |
| Salmon | 4,9 |
| Beef | 2 |
| Eggs | 1,1 |
| Milk | 0,4 |

Causes of vitamin B12 deficiency
Underconsumption
-
-
- Vegetarianism and veganism: Because vitamin B12 is synthesized exclusively by microorganisms and accumulates in animal tissues, people who exclude animal products from their diet are at risk of deficiency.
- Malnutrition: Individuals with malnutrition or eating disorders may develop vitamin B12 deficiency.
-
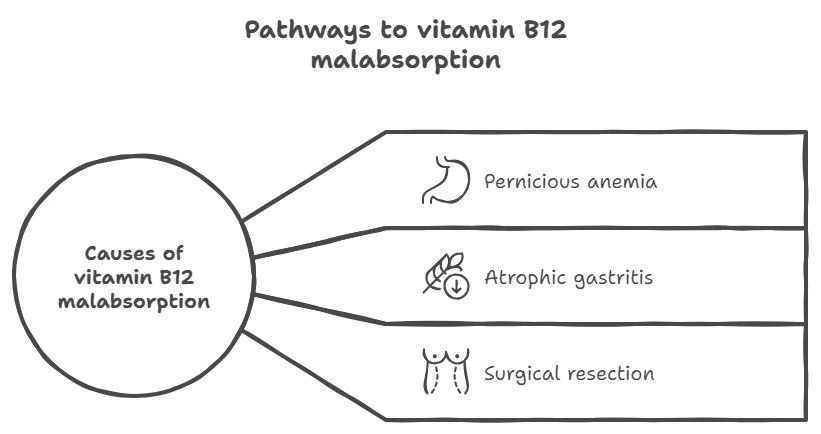
Absorption disorder
-
-
- Pernicious anemia : An autoimmune disease in which antibodies destroy gastric parietal cells, reducing the production of intrinsic factor Kasl, which is necessary for the absorption of vitamin B12.
- Atrophic gastritis: Decreased numbers of parietal cells and decreased stomach acidity impair the release of vitamin B12 from food.
- Gastric or ileum resection: Surgical removal of parts of the GI tract may reduce the area of vitamin B12 absorption.
-
-
Medications
-
-
- Metformin: Long-term use of metformin in type 2 diabetes is associated with decreased absorption of vitamin B12.Proton pump inhibitors and H2-receptor antagonists: Reduce gastric acidity, which may prevent the release of vitamin B12 from food proteins.
-
Interesting fact
Consumption of large amounts of alcohol can damage the gastric and intestinal mucosa, which negatively affects the absorption of vitamin B12.
Neurological manifestations of deficits
Vitamin B12 deficiency leads to demyelination of nerve fibers in the central and peripheral nervous system. This is due to the accumulation of methylmalonic acid and homocysteine, which have a neurotoxic effect.
Peripheral neuropathy
-
-
- Symmetrical paresthesias: Tingling and numbness in the extremities.
- Decreased vibration and proprioceptive sensitivity: May lead to impaired coordination of movements.
-
Spinal degeneration
-
- Funicular myelosis: Lesion of the posterior and lateral columns of the spinal cord resulting in muscle weakness, spasticity and ataxia.
Cognitive and psychiatric disorders
-
-
- Dementia: Memory impairment, cognitive decline.
- Psychosis and depression: Mood changes, hallucinations.
-
Optic neuropathy
-
- Decreased visual acuity: Due to demyelination of the optic nerve.
Table 2: Neurological symptoms of vitamin B12 deficiency
| Symptom | Description |
|---|---|
| Paresthesias | Tingling and numbness in the extremities |
| Ataxia | Balance and coordination disorders |
| Dementia | Deterioration of memory and cognitive function |
| Optic neuropathy | Decreased visual acuity |
| Depression | Low mood, apathy. |
Interesting fact
Neurologic symptoms can develop with normal hemoglobin levels and absent anemia, making vitamin B12 deficiency a “masked” pathology.

Diagnosis and treatment
Diagnosis
-
-
- Determination of serum vitamin B12 levels: Normal values are usually 200-900 pg/mL. Values below 200 pg/mL are considered a deficiency.
- Methylmalonic acid (MMC) and homocysteine levels : Elevated MMC and homocysteine levels are more sensitive markers of vitamin B12 deficiency.
- Intrinsic factor antibodies: For diagnosis of pernicious anemia.
-
-
Differential diagnosis
-
-
- Folic deficiency: May have similar hematologic manifestations, but neurologic symptoms are usually absent.
- Genetic diseases: Some inherited metabolic disorders may mimic vitamin B12 deficiency.
-
Treatment
-
-
- Parenteral administration: Injections of cyanocobalamin intramuscularly or subcutaneously according to a regimen (e.g., 1000 mcg daily for a week, then weekly and monthly).
- Oral administration: High doses (1000-2000 mcg/day) may be effective even if absorption is impaired.
- Therapy monitoring: Assessment of clinical improvement and normalization of laboratory values.
-
-
Interesting fact
Some studies suggest that nasal gels and sprays with vitamin B12 may be an effective alternative to injections.

Prevention
-
-
- Dietary Guidelines : Increase consumption of foods rich in vitamin B12, especially for vegetarians and vegans.
- Screening of risk groups: Elderly people, patients with gastrointestinal diseases, pregnant women.
- Food enrichment: Adding vitamin B12 to foods such as cereals and plant-based dairy alternatives.
-
-
Conclusion
Vitamin B12 deficiency is a serious medical problem because of its wide-ranging effects on the nervous system and hematologic parameters.
Early diagnosis and timely initiation of treatment are critical to prevent irreversible neurologic damage.
Health care providers should be aware of the diverse clinical manifestations of vitamin B12 deficiency and include it in the differential diagnosis for appropriate symptoms.
List of references
-
- O’Leary F., Samman S. Vitamin B12 in health and disease. Nutrients. 2010;2(3):299-316.
-
- Allen L.H. Causes of vitamin B12 and folate deficiency. Food Nutr Bull. 2008;29(2 Suppl)
-
- Herrmann W., Obeid R. Causes and early diagnosis of vitamin B12 deficiency. Dtsch Arztebl Int. 2008;105(40):680-685.
-
- Selhub J. Public health significance of elevated homocysteine. Food Nutr Bull. 2008;29(2 Suppl)
-
- Pawlak R., Parrott S.J., Raj S., Cullum-Dugan D., Lucus D. How prevalent is vitamin B12 deficiency among vegetarians? Nutr Rev. 2013;71(2):110-117.
-
- Toh B.H., van Driel I.R., Gleeson P.A. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448.
-
- de Jager J., Kooy A., Lehert P., et al. Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: randomised placebo controlled trial. BMJ. 2010;340
-
- Matoori S., Leroux J.C. Recent advances in the treatment of hyperhomocysteinemia. Curr Drug Targets. 2010;11(11):1461-1473.
-
- Healton E.B., Savage D.G., Brust J.C., Garrett T.J., Lindenbaum J. Neurologic aspects of cobalamin deficiency. Medicine (Baltimore). 1991;70(4):229-245.
-
- Lindenbaum J., Healton E.B., Savage D.G., et al. Neuropsychiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis. N Engl J Med. 1988;318(26):1720-1728.
-
- Hvas A.M., Nexo E. Diagnosis and treatment of vitamin B12 deficiency–an update. Haematologica. 2006;91(11):1506-1512.
-
- Sharabi A., Cohen E., Sulkes J., Garty M. Replacement therapy for vitamin B12 deficiency: comparison between the sublingual and oral route. Br J Clin Pharmacol. 2003;56(6):635-638.
-
- Carmel R., Green R., Rosenblatt D.S., Watkins D. Update on cobalamin, folate, and homocysteine. Hematology Am Soc Hematol Educ Program. 2003:62-81.
About the Author